
Becky Foster and Simon Satchell received a three-year BHF grant to investigate endothelial glycocalyx restoration. Principal Investigator Becky explains:
Proteinuria (protein within the urine) is an independent risk factor for cardiovascular disease. This is not only relevant for patients with kidney disease, but also for five per cent of the general population who have low-level proteinuria. A twofold increase in proteinuria increases risk of cardiovascular mortality by 30 per cent.
If we knew how proteinuria is linked to vascular damage, we would potentially be able to treat these patients to prevent vascular disease.
Proteinuria begins in the filtering microvessels that form the glomerulus in the kidney. The microvessel wall is a specialised filtration barrier made up of endothelial cells, a glomerular basement membrane and epithelial cells (podocytes). Podocyte damage is often key to major glomerular protein leakage. A proteoglycan-rich endothelial glycocalyx (eGlx) layer lines all blood vessels. Damage to eGlx leads to increased vascular leakage around the body, which can progress to vascular disease.
We have also shown that, in conditions of proteinuria, eGlx is also damaged in non-kidney blood vessels, and that this is associated with increased vascular leak. Heparanase is an enzyme that is upregulated in conditions of proteinuria by podocytes and also induces eGlx damage.
Our study will address our novel research question, that podocyte-induced heparanase expression causes vascular eGlx damage in proteinuric disease.
From this project, we will know whether heparanase upregulation by podocytes induces vascular damage, whether podocyte damage in proteinuria causes eGlx vascular damage and whether this is dependent upon heparanase. We will also use a clinically relevant heparanase inhibitor, which can be used to drive translat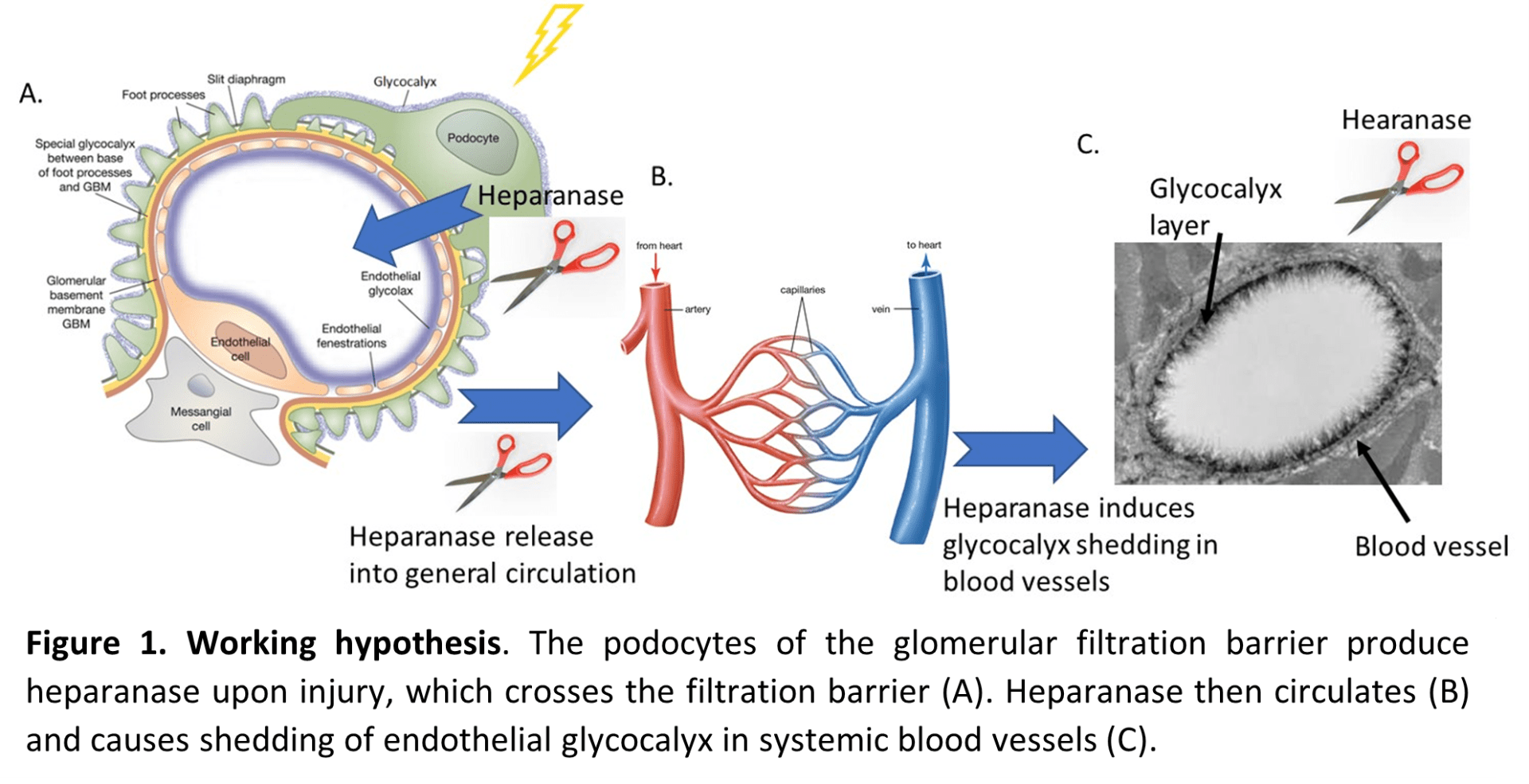 ion into the clinic for these patients.
ion into the clinic for these patients.
This post first appeared in the March 2021 BHI Newsletter